Welcome to PEMAZYRE Finland
This website is intended for healthcare professionals located in Finland.
Please login:

What's on this site:
Mechanism of action
Efficacy
Safety profile
Dosing and administration schedule
FGFR2 fusion
testing
Cholangiocarcinoma (CCA) & PEMAZYRE self-directed learning
A self-directed learning material to complete in your own time. With the learning module, you can learn about the unmet needs in CCA, discuss the need for molecular profiling for early patient identification and learn more about PEMAZYRE.
FGFR2 fusion testing
Discover about FGFR2 fusions in patients with CCA.

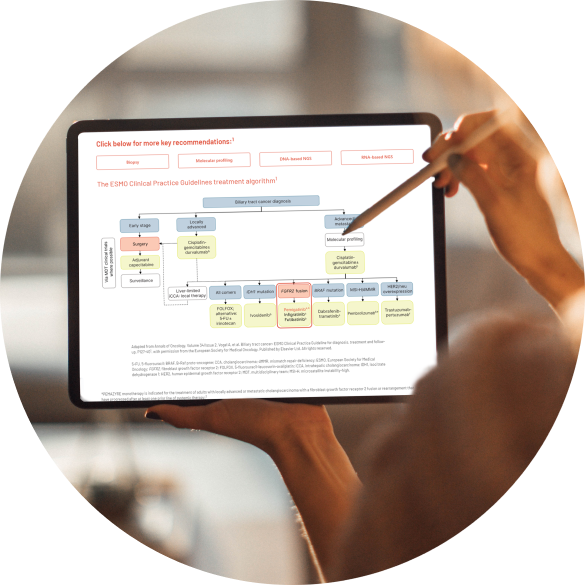
ESMO guideline recommendations
Discover more about ESMO guideline recommendations for patients with CCA.
Marketing authorisation holder:
Incyte Biosciences Distribution B.V.
Paasheuvelweg 25
1105 BP Amsterdam
Netherlands
If you would like to request further medical information, please visit:
https://www.incyteglobalmedicalinformation.com/